The Future of Epidemiology
Members of the Epinor advisory board,
friends and colleagues.
First, let me express my thanks for being invited to this seminar on the future of epidemiology. The future is not for us to see until it has become the past that is, but as Winston Churchill phrased it; “The farther backward you can look, the farther forward you are likely to see.” I appreciate his use of the word likely. We will, in this debate, I hope, talk about probable scenarios, assess their risks and consequences, and maybe identify future epidemiological research avenues. And I will look backward to get us on track.
My teacher at LSHTM, and later faculty colleague at the international traveling circus on cardiovascular epidemiology and prevention, the late Professor Geoffrey Rose, attended the first meeting of the Norwegian Epidemiological Association in 1990. He greeted us with these opening words «The end result of epidemiologists´ research is commonly a publication in an epidemiological journal, which is then read by other epidemiologists. We have become a closed community, and the effect is to encourage work which is methodologically interesting rather than of practical importance».
He then went back to 1850 and pointed at the 12 physicians who formed the Epidemiological Society of London. They had understood that hospital care was an incomplete answer to common diseases. To control such problems, one had to recognize their causes and origins. The last two years have demonstrated how true this is. And also, that we cannot focus only at the individual level. We need to be concerned equally with causal pathways at the societal level as well as pathogenesis and causality at the molecular level. SARS-CoV-2 was a new player in the molecular field. The stage, however, was set by social and economic differences. The pandemic was not a great equalizer. Only rarely have pandemics struck equally across socioeconomic categories.
Epidemiology attempts to describe disease occurrence, and from the observations in the past, predict the future. But the discipline is also aiming at identifying causes, heavily involved in etiological thinking to develop an appropriate intervention. When possible, one should add. Disease occurrence, or rather frequency is not very sexy, as long as it is flat. Only when it varies, between populations and over time will we start getting interested. That was what John Graunt reported on the social distribution of excess deaths in London of the plague in the 17th century. Excess deaths, still a highly relevant measure when assessing the development of an ongoing pandemic.
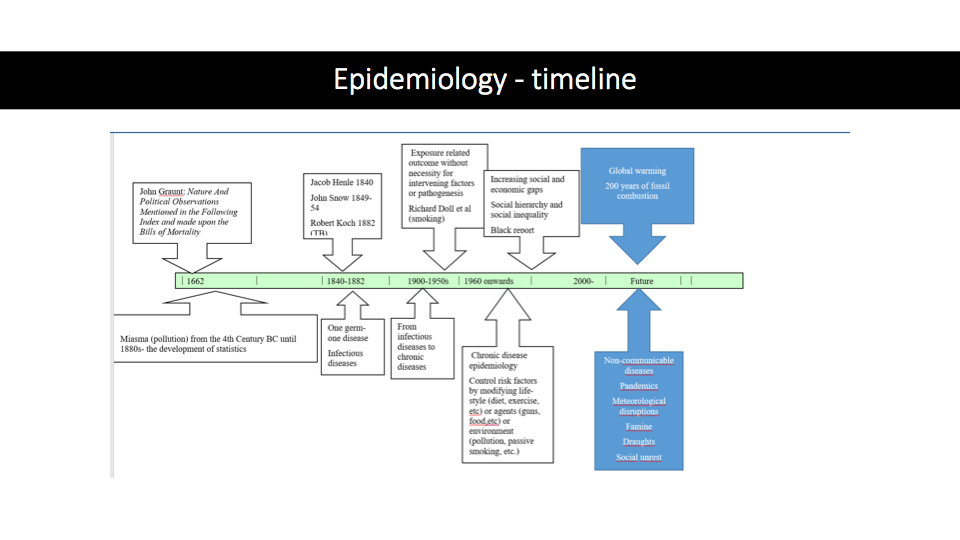
The figure above depicts different leading theories on the causes of diseases. The specific causes, however, were more in dark. Miasma, literally pollutants, were thought to spread disease, and sanitary statistics from the city slums showed how mortality clustered in poor areas. This only supported the idea that the miasma of foul emissions from dirt and garbage caused fatal diseases. The solution was closed drainage and sewage systems, garbage collection, and public baths. The pathogenic theory was wrong, but the means were effective. The germ theory with its emphasis on one factor-one disease turned medicine into a more mechanistic way of thinking. The appropriate responses were to isolate, vaccinate and treat those affected, whereas social and economic factors contributing to the disease occurrence were more or less neglected. The declining importance of infectious diseases paved the way for chronic diseases such as cardiovascular diseases and certain cancers during the 1930s. They were later to be categorized as non-communicable disorders (NCD), and their increasing importance was considered as emerging epidemics. But more importantly, one realized that the concept of one agent- one disease, was not sufficient to explain the variation. Social class and economic conditions emerged as important contributors, exemplified among others by the publication of the Black report in the early 1980s. Today we face all of these different stages in thinking about disease etiology. The infectious diseases have shown that we are unprepared, the NCDs are taking their share of the health care resource, and we are looking into the abyss of a rapidly changing climate. We know some of the consequences, drought, famine, social unrest, pandemics, but also direct effects on cardiovascular disorders and certain cancers.
The question is not what the future will be. We know from the past the likely scenarios. The question is how do we act, as epidemiologists in assessing the risks and conveying the message to the appropriate public health authorities and politicians.
I have not mentioned newer research methods; advanced causal inference, the use of Mendelian Randomization, Directed Acyclic Graphs, Big Data, and Artificial Intelligence. Those are exciting and promising techniques, but not the solution to what lies ahead. The ball is in your field.
Thank you.
https://uit.no/tavla/artikkel/667633/the_future_of_epidemiology_2021
